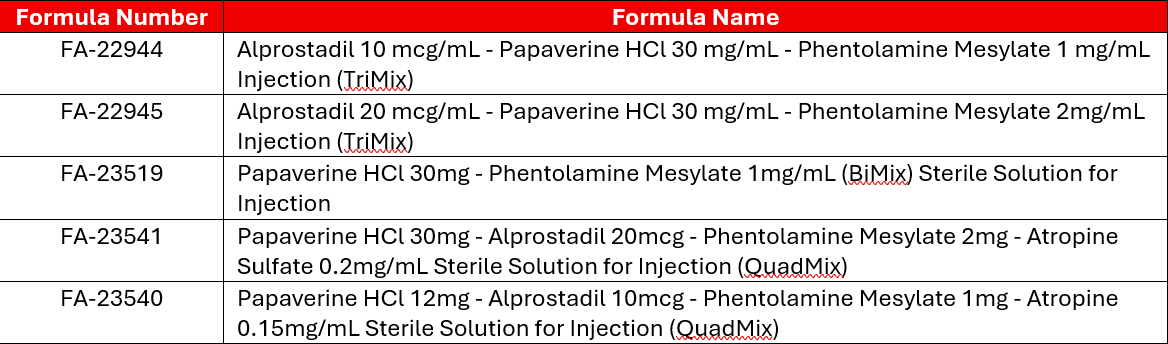
Intracavernosal medications are commonly used for erectile dysfunction refractory to oral medications. In addition to commercially available alprostadil, compounded combinations of alprostadil, phentolamine mesylate, and papaverine HCl (better known as Tri-mix) or alprostadil, phentolamine mesylate, papaverine HCl, and atropine sulfate (better known as Quad-mix) are sometimes prescribed. Subsets of phentolamine mesylate and papaverine HCl without alprostadil (better known as Bi-mix) are also sometimes used. In this blog post, we’ll briefly review the mechanisms of action on each component as well as data on concentrations in combination.
Alprostadil
Alprostadil is a prostaglandin that induces vasodilation and relaxes smooth muscle. The commercially available product is typically dosed at up to 60mcg per dose, starting at 2.5mcg and titrating up.1 Many patients (approximately 20-38% depending on the type of erectile dysfunction) find benefit at small initial doses at less than 2mcg, for those that increase the dose, they noted that median effective dose was 3-5mcg depending on type of erectile dysfunction.2
Another study found a 90% efficacy at a dose of 20mcg.3 In terms of onset, studies have found a wide range of onset time ranging from 12 to 44 minutes in some literature with duration up to 100 minutes.2 Some information notes that higher doses may be associated with a longer duration of erection.3 Generally recommendations are to inject alprostadil 10 -30 minutes before intercourse for best effect. Combination products in Tri-mix use slightly lower doses at 2.5mcg up to 20mcg per dose depending on the product.2,5
Papaverine HCl
Papaverine HCl is a nonselective phosphodiesterase-5 (PDE-5) inhibitor that acts via increasing arterial flow and decreasing venous outflow.6,7 Limited studies on papaverine intracavernosal injection found onset of erection varied based on expected cause of impotence. Studies in generally healthy volunteers found onset of erection 10 minutes post-injection and lasting for over an hour, but depending on type of impotence response could be delayed and shortened.6
As a solo agent papaverine is administered in a wide range of doses up to 60mg, though, a typical starting dose is around 15mg. The package insert for commercially available products intended for intracavernosal injection (not currently available in the US) also lists expected erection onset at 10 minutes and note that it may last from one to several hours.8,9
Phentolamine Mesylate
Phentolamine mesylate is a nonselective alpha-adrenergic receptor antagonist that blocks sympathetic stimulation of smooth muscle.7 Phentolamine mesylate is generally not used as a solo agent for erectile dysfunction. Combination products in Tri-mix or Bi-mix typical dose phentolamine mesylate between 0.2-2mg per injection.2,5 Tri-mix preparations containing phentolamine mesylate typically have a quick onset within 10 to 15 minutes.10
Atropine Sulfate
Atropine sulfate is not typically used as a solo agent for management of erectile dysfunction, it is sometimes used in “Quad-mix” combinations with alprostadil, papaverine, and phentolamine. Typical concentration is 0.1-0.2mg/mL.11,12
Bi-Mix (Phentolamine Mesylate/Papaverine HCl)
Though three drug tri-mix combinations are more common, studies have evaluated combination papaverine HCl and phentolamine mesylate without alprostadil as well. One study on combination phentolamine mesylate 1mg and papaverine HCl 30mg/mL found benefit with injection volumes of 0.1-0.4mL in all patients in this small study.13 Though bi-mix appears to be effective for erectile dysfunction, its benefit over alprostadil alone is unclear.
One study comparing alprostadil at 20mcg per dose vs bi-mix (papaverine HCl 30mg, phentolamine mesylate 1mg) found that both treatments were equally effective at producing an erection.15,16 Another comparative study looking at tri-mix vs bi-mix noted tri-mix to be superior. This study looked at 20 patients with reported impotence over two sessions and noted 73% of patients reported achieving a full erection with tri-mix compared with just 28% of the bi-mix group. Duration of action was longer in the tri-mix group as well, with average duration being 57 minutes vs 33.6 minutes in the tri-mix and bi-mix groups respectively.14
Tri-Mix Studies
Tri-mix is typically considered if patients do not experience an adequate response to intracavernosal monotherapy. One study evaluating a high dose of alprostadil (40mcg/mL) vs papaverine 17.64mg, phentolamine 0.58mg, and alprostadil 5.8mcg/mL in patients who failed to respond to bi-mix found a much greater response rate in patients on tri-mix therapy (22% vs 50%) and a lower incidence of pain (41% vs 12.5%) in the tri-mix group as compared to the high dose alprostadil group.16,17
A separate study comparing alprostadil 20mcg to bi-mix (papaverine 30mg, phentolamine 1mg) to tri-mix (papaverine HCl 15mg, phentolamine mesylate 0.5mg, alprostadil 10mcg) noted significantly increased response in the tri-mix group as compared to alprostadil alone or bi-mix.15,16 With regards to the most effective concentrations of tri-mix, studies comparing alprostadil 2.5-10mcg, papaverine HCl 5-20mg, and phentolamine mesylate 1mg failed to detect a statistically significant difference in patient reported efficacy or preference between these strengths.5 Though tri-mix appears to be more effective and less associated with pain than alprostadil alone, studies have shown an increased risk of priapism with tri-mix treatment as compared to alprostadil alone.5
Though concentrations vary across studies, the most common ratio is phentolamine mesylate 1 (in mg), alprostadil 10 (in mcg), and papaverine HCl 30 (in mg).5 Bracketed stability studies published in IJPC have evaluated from alprostadil 5mcg, papaverine 15mg, phentolamine 0.4mg up to alprostadil 45mcg, papaverine 30mg, and phentolamine 5mg, suggesting good overall stability of these combinations.
Quad-Mix
For patients who do not have an adequate response to an escalated dose of tri-mix, limited studies have evaluated the addition of atropine sulfate to the traditional alprostadil/papaverine HCl/phentolamine mesylate mixtures. One study evaluating a mixture of papaverine HCl 12.1mg/mL, Alprostadil 10.1mcg/mL, phentolamine mesylate 1.01mg/mL, and atropine 0.15mg/mL dosed at 0.25 to 0.9mL per injection found a sufficient response in 95% of men.11
Though the ability of quad-mix to produce erections has been established, its benefit over tri-mix combinations is unclear. One study of papaverine HCl 50mg, alprostadil 10mcg, phentolamine mesylate 0.2mg with or without atropine 0.075mg did not report a statistically significant difference between groups, though, it should be noted that the atropine concentration used in this study was quite small.18
Notes on Administration:
- A fine 29 or 30 gauge, 5/16ths or 1/2in needle is typically used for injection
- Injection volume for intracavernosal injection is often small ranging from 0.1mL to a maximum of 1mL but typically much lower volumes (more like 0.1-0.25mL are used)
- Typical onset of action is between 5-15 minutes and can last up to an hour or two, erections lasting longer than 4 hours may require intervention (such as injection with phenylephrine vasoconstrictor)
- Typical recommendation is to use no more than three times weekly consistent with commercially available alprostadil for intracavernosal injection
References:
1. Caverject (alprostadil) [package insert]. Pharmacia and Upjohn Company. New York, NY. Updated May 2024. Accessed July 2025.
2. Leslie SW, Jain A, Iqbal OA. Alprostadil. [Updated 2025 Feb 6]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK542217/
3. Shokeir AA, Alserafi MA, Mutabagani H. Intracavernosal versus intraurethral alprostadil: a prospective randomized study. BJU Int. 1999 May;83(7):812-5. doi: 10.1046/j.1464-410x.1999.00021.x. PMID: 10368203.
4. Linet O, Ogrinic F. Efficacy and safety of intracavernosal alprostadil in men with erectile dysfunction. N Engl J Med. 1995; 334: 873-877.
5. Seyam R, Mohelden K, Akhras A, Rashwan H. A Prospective Randomized Study to Optimize the Dosage of Trimix Ingredients and Compare Its Efficacy and Safety with Prostaglandin E1. International Journal of Impotence Research. 2005: 17(4):346-53
6. Virag R, Frydman D, Legman M, Virag H. Intracavernous Injection of Papaverine as a Diagnostic and Therapeutic Method in Erectile Failure. Angiology. 1984;35(2):79-87. doi:10.1177/000331978403500203
7. Sami S, Stern N, Di Pierdomenico A, Katz B, Brock G. Erectile Dysfunction: A Primer for in Office Management. Medical Sciences. 2019; 7(9):90. https://doi.org/10.3390/medsci7090090
8. Ghafoori, M., Hoseini, K. & Shakiba, M. Comparison of one-side and bilateral intracavernosal papaverine injection on a Doppler study of the penis. Int J Impot Res 21, 382–386 (2009). https://doi.org/10.1038/ijir.2009.50
9. https://www.medsafe.govt.nz/profs/datasheet/d/dblPapaverineHydrochlorideinj.pdf. Papaverine Hydrochloride [package insert]. Version: pfdpapai10421
10. Said SZ, Nasser TA, Ayad M, Motawi AT. Evaluation of the sensitivity of different doses of vasoactive drugs in diagnosing erectile dysfunction in impotent patients: a prospective case-control study. Cent European J Urol. 2021;74(1):109-115. doi:10.5173/ceju.2021.00042.R1
11. Montorsi F, Guazzoni G, Bergamaschi F, Ferini-Strambi L, Barbieri L, Rigatti P. Four-drug intracavernous therapy for impotence due to corporeal veno-occlusive dysfunction. J Urol. 1993 May;149(5 Pt 2):1291-5. doi: 10.1016/s0022-5347(17)36371-1. PMID: 7683061.
12. Fayez AH, El-Khayat Y, Hosny H, Zaki S, Shamloul R. A study of the possible effects of repeated intracorporeal self-injection of vasoactive drugs in patients with elevated end diastolic velocity during pharmacopenile duplex ultrasonography. Cent European J Urol. 2013;66(2):210-214. doi:10.5173/ceju.2013.02.art25
13. Fein RL. Intracavernous medication for treatment of premature ejaculation. Urology. 1990 Apr;35(4):301-3. doi: 10.1016/0090-4295(90)80149-h. PMID: 1690937.
14. Shenfeld O, Hanani J, Shalhav A, Vardi Y, Goldwasser B. Papaverine-phentolamine and prostaglandin E1 versus papaverine-phentolamine alone for intracorporeal injection therapy: a clinical double-blind study. J Urol. 1995 Sep;154(3):1017-9. PMID: 7637045.
15. Khera M, Goldstein I. Erectile dysfunction. BMJ Clin Evid. 2011;2011:1803. Published 2011 Jun 29.
16. Ribe N, Rajmil O, Bassas L, et al. Response to intracavernous administration of 3 different drugs in the same group of patients with erectile dysfunction. Arch Esp Urol 2001;54:355–359.
17. Bechara A, Casabe A, Cheliz G, et al. Prostaglandin E1 versus mixture of prostaglandin E1, papaverine and phentolamine in nonresponders to high papaverine plus phentolamine doses. J Urol 1996;155:913–914
18. Sagari P, Teloken C, Souto C. atropine role in the pharmacological erection test: study of 228 patients. The Journal of Urology. 1997; 158(5): 1760-1763.
19. Linet O, Ogrinc F. Efficacy and Safety of Intracavernosal Alprostadil in Men with Erectile Dysfunction. N Engl J Med. 1996; 334(14): 873-877.